
Case Report | DOI: https://doi.org/10.31579/2692-9392/026
1 Bawaskar Hospital and Clinical research center, Mahad, Raigad Maharashtra, India, 402301
*Corresponding Author: Himmatrao saluba bawaskar, Bawaskar Hospital and Clinical research center, Mahad, Raigad Maharashtra, India
Citation: Himmatrao S Bawaskar., Pramodini H. Bawakar., (2021) Primary Bilateral Papilledema due Myxedema. J. Archives of Medical Case Reports and Case Study, 4(1); DOI:10.31579/2692-9392/026
Copyright: © 2021 Himmatrao Saluba Bawaskar, This is an open access article distributed under the Creative Commons AttributionLicense, which permits unrestricted use, distribution, and Reproduction in any medium, provided the original work is properly cited.
Received: 09 February 2021 | Accepted: 12 March 2021 | Published: 17 March 2021
Keywords: hypothyroidism;cerebrospinal fluid; thyroid hormone
Hypothyroidism is a highly prevalent disorder and can substantially impact the well-being of an individual. Till date there is no single accurate optimal target zone for thyroid stimulating hormone concentration that exists in the context of replacement of thyroid hormone. Due to the gradually progressive nature and insidious onset of disease, it often remains unrecognized
Hypothyroidism is a highly prevalent disorder and can substantially impact the well-being of an individual. Till date there is no single accurate optimal target zone for thyroid stimulating hormone concentration that exists in the context of replacement of thyroid hormone. Due to the gradually progressive nature and insidious onset of disease, it often remains unrecognized. Deposition of myxomatous tissue results in oedema, and in neuro-vascular compression which can then affect the venous and cerebrospinal fluid (CSF) drainage [1].
On 15th October 2019, a 24 year-old female reported at the out-patient department with complaints of diminution and blurring of vision, since the last 6 days. She noticed that while fixating on an object, it gradually became more clearer with the passage of time, suggestive of delayed accommodation. She complained of having irregular menstruations, since the previous 18 months, paresthesia in both hands and feet since one year; recurrent persistent cramping in calf, chest and abdominal muscles; once she developed severe cramps in the masseter muscles. She developed hoarseness of voice, weakness, laziness and her mother also complained that she snored loudly during her sleep. She could easily pull out a bunch of scalp hairs; the skin over her palms and soles had become cold and dry over the previous year; she suffered from recurrent upper respiratory tract infections. The patient denied having had any episodes of headache, vomiting, giddiness and convulsions. She also denied having a family history of a similar illness. She was seen by various doctors and consumed multivitamins and diuretics for quite some time. On examination, she weighed at nearly 63kgs and as per her previous recorded weight, there was an increment of almost 10 kilos, despite her following a strict diet for the previous 18 months. The young lady had brittle hair, puffed face (appendix A), swelling of both her feet (appendix B). Her speech was slow and slurred, with slow relaxation of ankle jerks (appendix video 1). She had slow relaxation and contraction of iris to light response (appendix video 2a). Also, she had extensive fungal infection over her abdomen. Skin was cold, pulse was 88 per minute and low volume, blood pressure was 110/80 mm hg. In both the eyes, there was a delay in finger counting. Fundus examination revealed bilateral papilledema with obscuration of the disc vasculature, prominent nerve fibre layer elevation, venous congestion and absence of late cup and venous pulsation with dilated tortuous vessels, (Figure-1a arrow). Laboratory investigations showed haemoglobin at 10.2g/dl, platelet count at 82,000/ul, LDL cholesterol at 132.50mg/dl (normal= 8-100), total T-3 at 0.5(normal=1.3-3.1), T4 at 7.7(normal=66.181), TSH>100microIU/ml(normal=0.33-5.5) and the thyroxin peroxidase antibodies were at 380 IU/ml (normal=0- 5.6). Radiological assessment with an MRI brain revealed a normal scan with no sign of raised intracranial pressure (appendix MRI of brain). Electrocardiogram(Figure-1b) dated 15th October 2019 revealed a heart rate of 86 per minute, low voltage, total sum of R wave in limb leads I+II+III = 8.5mm(n>15mm) , with low T waves. She was put on levothyroxine 100ug daily on an empty stomach and then gradually the dose was raised to 125ug per day. After 15 days of starting treatment, her vision was improved enough to enable easy counting of figures. ECG dated 23rd December (Figure-1b) showed her heart rate as 83 per minute, total sum of R waves in limb leads voltage was I+II+III= 22 mm Hg. Her extremities became warm, the hoarseness in her voice reduced and so did her laziness and snoring during sleep. She had lost a little over 3 kgs of weight. She was re-evaluated on 27th December 2019 and found to have a reduction in papilledema. The vessels coming from disc became straight became prominence can be traced to the head of disc (figure 1aB).


ECG- 15 October 2019-Electrocardiogram heart rate 86 per minute , low voltage sum of total R waves in limb lead R wave I+II+III = 8.5mm(n>15mm) ( ECG 15th October) , with low T wave
ECG- 23 December 2019- ECG showed heart rate 83 per minute , sum of total voltage R waves in limb lead I+II+III= 22 mm .
Most recently she was assessed on 12th June 2020, and by now she had lost over 8kilos; had an overall reduction in puffiness over her face (appendix c); pupils were reacting vigorously to light (appendix video 2b); TSH was measured at 0.144 IU; papilledema had completely resolved (figure 1aC).
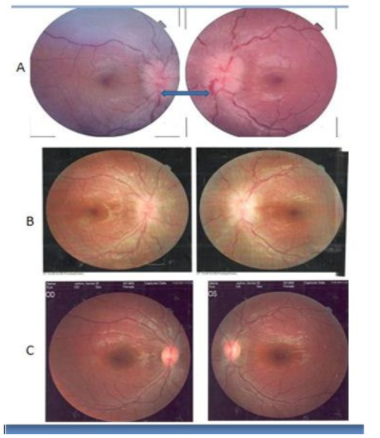
Vision had totally improved in both her eyes to 6/6. The dose of levothyroxine was now reduced to 100ug.
Dear Editorial Team, Clinical Medical Reviews and Reports. My experience with the journal was highly positive. The peer-review process was rigorous, constructive, and completed in a timely manner. The reviewers provided valuable comments that helped improve the quality and clarity of our manuscript. The editorial office was professional, responsive, and supportive throughout all stages of the publication process. Communication was clear and efficient, and any questions were addressed promptly. Overall, I found the journal to maintain high scientific standards and an excellent publication workflow. I would be pleased to consider submitting future work to this journal. Best wishes from, Elena Popa.

It was my pleasure to submit my testimonial concerning the Reviewer Board of our Scientific Journal “Brain and Neurological Disorders”. The Reviewers focused on some modifications and their contribution was helpful. The ladies of our Editorial Office were also supported my efforts. It was my honor to have such a co-operation and I am looking forward for more collaboration.

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Thank you for the speedy and efficient peer review process. I appreciate the fact that your peer reviewers do not take months to respond like with some other journals. I would also like to thank the editorial office for responding quickly to my questions. It is an excellent journal. I plan to submit more manuscripts in the future. Best wishes from, Robert W. McGee

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Working with you and your team on our recent publication in JCRR has been a truly wonderful and enjoyable experience. The responses were prompt, and the reviewers were patient, constructive, and highly professional. One reviewer in particular gave me the feeling that a professor was carefully reading and commenting on my coursework, which was deeply touching. The entire process was straightforward and hassle‑free, with no tedious online forms to complete. I highly recommend this journal. Best wishes from, DR Aibing Rao, Head of R&D

I Appreciate the Opportunity to Share my Experience with the Journal of Clinical Research and Reports. The peer review process was timely and constructive, and the feedback provided helped improve the quality of our manuscript. The editorial office was professional, responsive, and supportive throughout the process, ensuring smooth communication and efficient handling of the submission. Overall, it was a positive experience collaborating with your team.

Dear Mercy Grace, Editorial Coordinator of Obstetrics Gynecology and Reproductive Sciences, We would like to express our gratitude for your help at all stages of publishing and editing the article. The editors of the magazine answer all the necessary questions and help at every stage. We will definitely continue to cooperate and publish other works in the Obstetrics Gynecology and Reproductive Sciences! Best wishes from, Alla Konstantinovna Politova,
